
Pressure Guidewires, 2nd Generation Fiber Optic Sensor

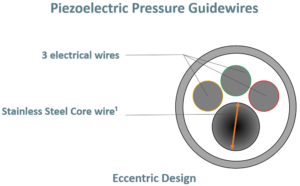
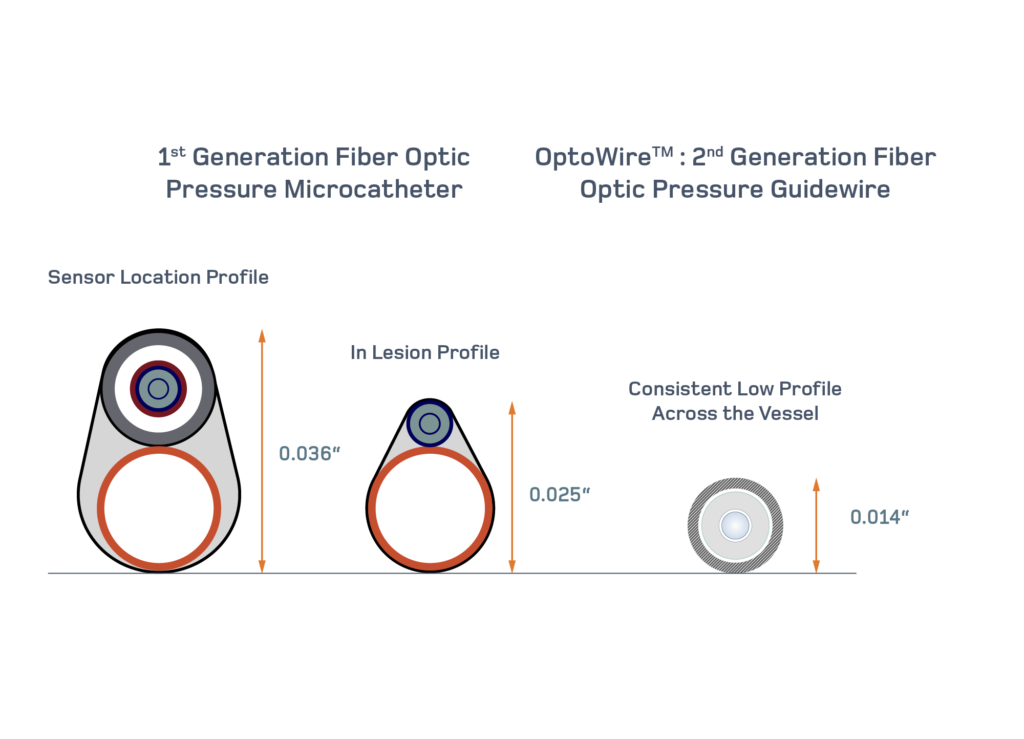
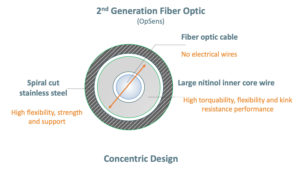
The OptoWire is a pressure guidewire, powered by FidelaTM, a 2nd generation fiber optic sensor. It has a design and performance that mimic very closely the design of a workhorse guidewire, making complex vessel navigation possible and predictable.
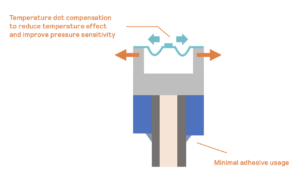
Additionally, the 2nd generation fiber optic sensor provides accuracy in the extreme conditions so physicians can use the same device to diagnose multiple segments ad arteries without worrying about losing accuracy.
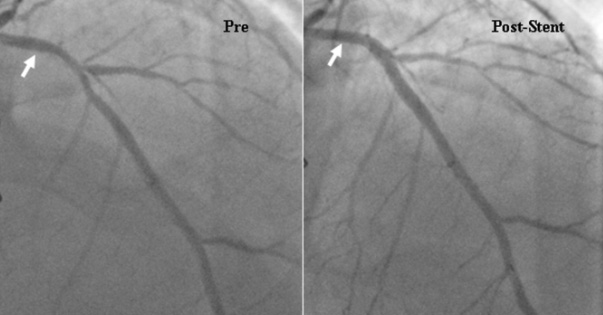
Finally, this technology allows physicians to disconnect and reconnect easily to measure, perform PCI and confirm the improvement after the stent is implanted.
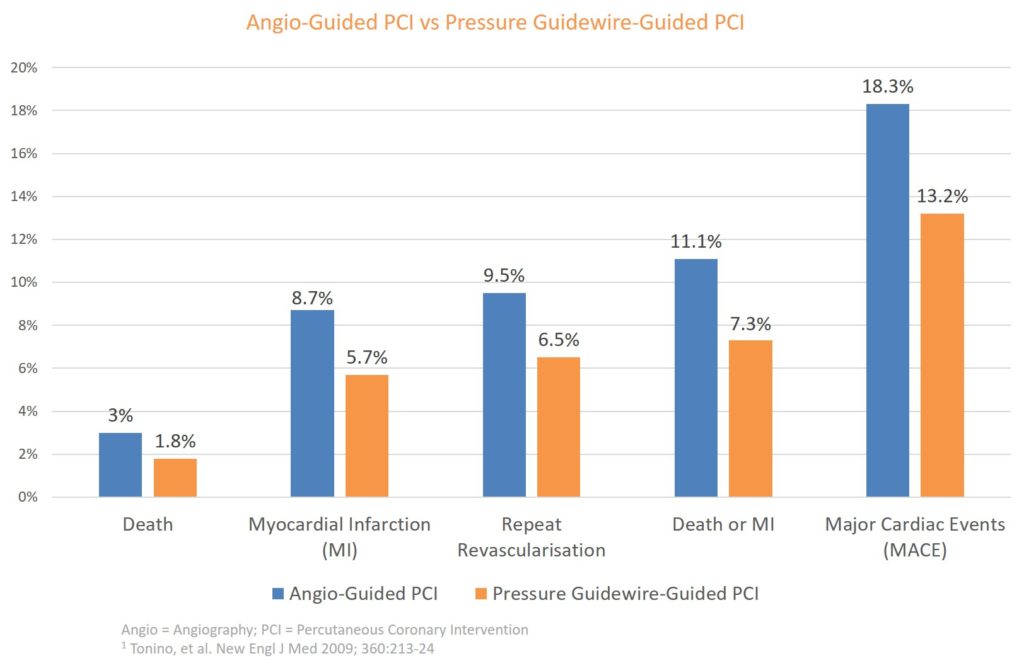
This last step could not be performed routinely before and has been reported to improve long-term clinical outcomes in several studies7,8.
Resting Indices
 We could not conclude this section without mentioning resting indices. FFR has been the gold standard in coronary physiology and requires hyperemia induced by drug such as adenosine to make the diagnosis. New indices that can be performed without the use of drugs have now come to market and have been proven to provide a good alternative to FFR9,10
Although they are much faster and easier to use, the scale to make a decision to treat is now narrower with an FFR cutoff value of 0.80 while the cutoff value for most resting indices is 0.89. In other words, while FFR provides 20 units to make a decision, resting indices provide only 11. The use of resting indices requires extreme accuracy, which makes the OptoWire perfectly suited for this kind of measurement. The OptoWire and OpSens diastolic pressure ratio (dPR) indice allows physicians to make several measurements, track the pressure variation across the artery (pullback) and assess pre-and post PCI with high confidence in the results’ accuracy.
The OptoWire brings physicians the possibility to diagnose and treat their patients with confidence.
We could not conclude this section without mentioning resting indices. FFR has been the gold standard in coronary physiology and requires hyperemia induced by drug such as adenosine to make the diagnosis. New indices that can be performed without the use of drugs have now come to market and have been proven to provide a good alternative to FFR9,10
Although they are much faster and easier to use, the scale to make a decision to treat is now narrower with an FFR cutoff value of 0.80 while the cutoff value for most resting indices is 0.89. In other words, while FFR provides 20 units to make a decision, resting indices provide only 11. The use of resting indices requires extreme accuracy, which makes the OptoWire perfectly suited for this kind of measurement. The OptoWire and OpSens diastolic pressure ratio (dPR) indice allows physicians to make several measurements, track the pressure variation across the artery (pullback) and assess pre-and post PCI with high confidence in the results’ accuracy.
The OptoWire brings physicians the possibility to diagnose and treat their patients with confidence. 
{kind=link}
{kind=link}
{kind=link}
{kind=link}